What’s that concerning spike in the last years?
deleted by creator
Can the generally upward trend also be attributed to less women having kids? I know this is a factor.
Could there be an increase because of more and better screening? Without total case numbers >50 it’s kind of useless. Even with that number however it would need cause of death statistics as well. More and better and earlier screening always results in higher numbers of early positive, creating an upwards trend that could as well be positive as on it’s own it says nothing.
Agreed. I wonder how one controls for confirmation bias here? Maybe show another graph depicting screening rates, or a plot showing the introduction of newer and more accurate screening methodologies?
The race thing doesn’t really say much does it. Poorer people are less likely to be properly diagnosed or seek medical attention.
The race side does have something to do with it when you look at broader issues, which are not available in this data.
Such as: keloid sufferers are much more likely to have breast cancer. This is not a SES issue, but a genetic one. There are likely other issues involved, but either way, this is not complete data and needs further explanation.
My thought is that the huge decrease in screening during the pandemic is leading to more cases being caught now that things have resumed normal.
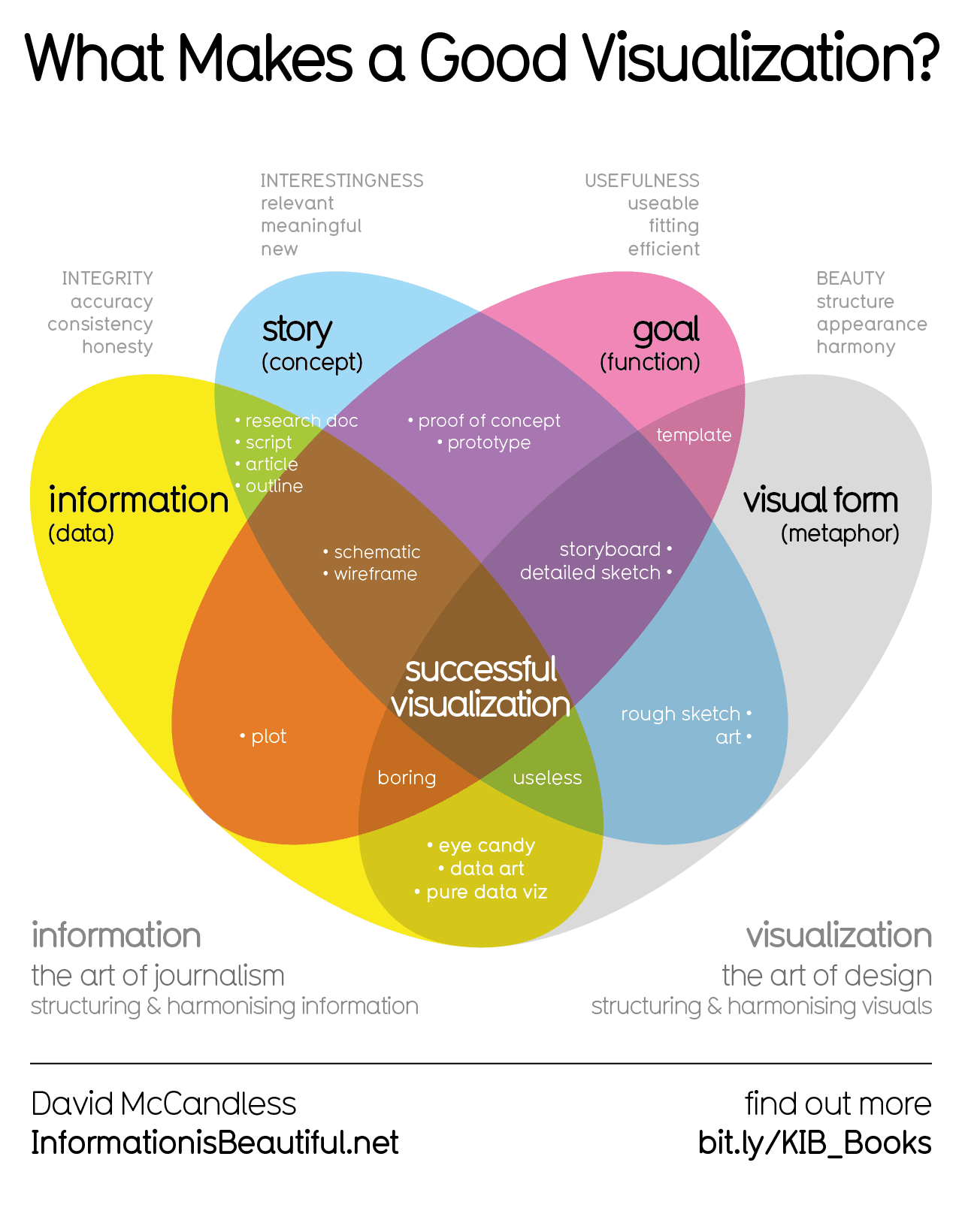
Its kind of nice to see a “by race” article showing that race is really not showing to be a factor in this study, every line looks the same.
Something that would be useful would be to know the stage of cancer being found. If it’s continually being an earlier find, that’s better.
Unfortunately, if it is like the findings for bowel cancers, I’m afraid it is just a general increase in cancer rates coming at us. Inflammation and disregulation of immune response is being seen in more and more pathologic tissues from plasticizers and other chemicals related to plastics.
Oh god, we need to do something.
WE NEED TO SAVE THE BOOBIES!
“By race” huh?!
Why the confusion?
If its the term race, that is what the original cancer.gov chart uses “raxe/ethnicity”. It’s not a term used in UK where I’m from - ethnicity is used - so I do find it odd from that viewpoint.
But Race/ethnicity is a very important health metric as different ethnicities have different risk levels for diseases, and it’s also an important way of checking for health inequalities.
For example the graph could be read as showing that young white and Asian women are at higher risk of breast cancer. Or it could be read that young black and Hispanic women with cancer are not being picked up early when young. Or many other interpretations. It’s very important data to collect and present in the health realm.
If race was important, they’d understand “Hispanic” is not a race.
Hispanic only means you speak Spanish natively. There are many white, indigenous, and black Hispanics, as well as Hispanics of East Asian descent, Middle Eastern descent, and more. Anya Taylor-Joy, Lupita Nyong’o, and Yalitza Aparicio have very different illnesses predispositions.
Hispanic people have also different socioeconomical levels, so it’s also absurd to throw people that are literally traveling to another country to be treated in reputated cities (e.g. Houston), who are not only capable of paying that but minimally bilingual, with people that crossed borders illegally, who often are illiterate or only got the opportunity to attend elementary school, and are doing a very dangerous journey with the idea that things will be easier in the United States. Two different worlds, two different health profiles. But no, “Hispanic”.
That is not how Hispanic is used in the dataset. Just read the methodology for crying out loud.Yes, “Hispanic (any race)”. And, as I said, it’s irrelevant statically as Hispanics do not share enough characteristics to be a homogenous group. Then you have “non-Hispanic” groups and “including Hispanic” races, which is nuts if you consider what I said.
Imagine you had a “Catholics (any race)” and then “Non-Catholic Whites”, “Whites (including Catholics)”, etc. That would be bordering discrimination because why are Catholics being segregated when other religions aren’t?
(I know why: because these “Catholics” are differentiated and not particularly well received in the United States due to illegal immigration).
Okay. That’s a very convincing analogy. Thanks for the thought out response. Forgive me for being rude.
I don’t think they mean hispanic as spanish speaking, but as the race resulting of the mingling of south american natives and europeans (mainly spaniards and portugueses). I feel the term hispanic is used in the USA since this group and the native spanish speakers overlap quite a bit. So it is not “Hispanic (any race)”, but more of " Hispanic american", who do share more genetic and ancestry similarities.
Also, when differenciating by race (we can debate wether this is legit or wether the predisposition to certain illnesses is minimal compared to income or quality of living, but that’s not what I am doing here), the socioeconomic differences are not relevant and appear in all groups. In that regard, “Hispano american” is not the only group with vast differences, but “White” and “Black” are very much riddled with it, but the thing is that for this study, it is not relevant, as it isn’t age (under 50) or state.
Now, what bothers me more is the “Asian/PI” category, I feel like that one has absolutely no basis. I’m guessing the sample was not big enough to qhave different cattegories, but that group feels very sloppy as a category by race.
Just to adress your first sentence: My first thought was that these groups most likely don’t go for checkups with the same frequency. On the socio economic dimensions of traits, Hispanics might define a homogeneous group.

{kind=link}